Early-life disease exposure and occupational status
Home > Early-life disease exposure and occupational status
by Martin Saavedra (Oberlin College and Conservatory)
This blog is part H of the Economic History Society’s blog series: ‘The Long View on Epidemics, Disease and Public Health: Research from Economic History’. This blog is based on the article ‘Early-life disease exposure and occupational status: The impact of yellow fever during the 19th century’, in Explorations in Economic History, 64 (2017): 62-81. https://doi.org/10.1016/j.eeh.2017.01.003

Like epidemics, shocks to public health have the potential to affect human capital accumulation. A literature in health economics known as the ‘fetal origins hypothesis’ has examined how in utero exposure to infectious disease affects labor market outcomes. Individuals may be more sensitive to health shocks during the developmental stage of life than during later stages of childhood. For good reason, much of this literature focuses on the 1918 influenza pandemic which was a huge shock to mortality and one of the few events that can be visibly observed when examining life expectancy trends in the United States. However, there are limitations to looking at the 1918 influenza pandemic because it coincided with the First World War. Another complication in this literature is that cities with outbreaks of infectious disease often engaged in many forms of social distancing by closing schools and businesses. This is true for the 1918 influenza pandemic, but also for other diseases. For examples, many schools were closed during the polio epidemic of 1916.
So, how can we estimate the long-run effects of infectious disease when cities simultaneously respond to outbreaks? One possibility is to look at a disease that differentially affected some groups within the same city, such as yellow fever during the nineteenth century. Yellow fever is a viral infection that spreads from the Aedes aegypti mosquito and is still endemic in parts of Africa and South America. The disease kills roughly 50,000 people per year, even though a vaccine has existed for decades. Symptoms include fever, muscle pain, chills, and jaundice, from which the disease derives its name.
During the eighteenth and nineteenth centuries, yellow fever plagued American cities, particularly port cities that traded with Caribbean Islands. In 1793, over 5,000 Philadelphians likely died of yellow fever. This would be a devasting number in any city, even by today’s standards, but it is even more so when considering that in 1790 that Philadelphia had a population of less than 29,000.
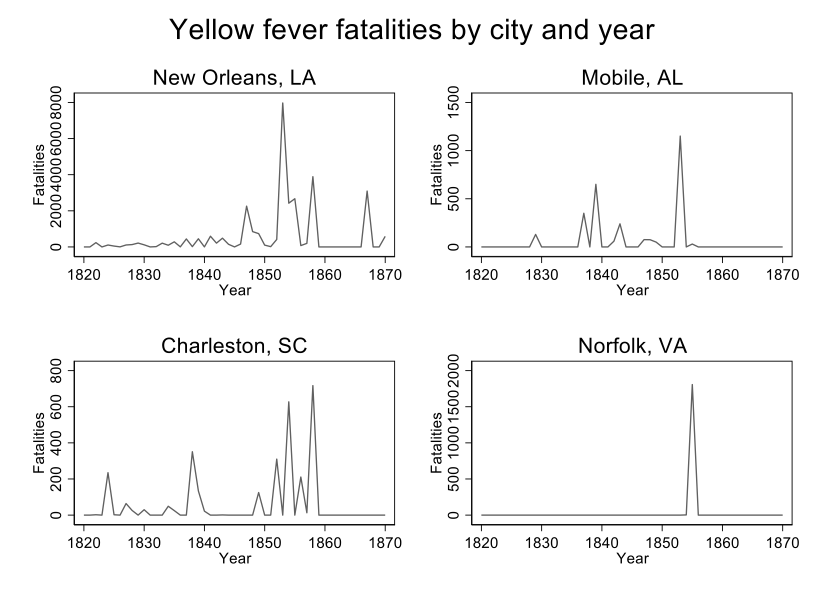
By the mid-nineteenth century, Southern port cities grew, and yellow fever stopped occurring in cities as far north as Philadelphia. The graph below displays the number of yellow fever fatalities in four southern port cities — New Orleans, LA; Mobile, AL; Charleston, SC; and Norfolk, VA — during the nineteenth century. Yellow fever was sporadic, devasting a city in one year and often leaving it untouched in the next. For example, yellow fever killed nearly 8,000 New Orleanians in 1853, and over 2,000 in both 1854 and 1855. The next two years, yellow fever killed fewer than 200 New Orleanians per year, then yellow fever come back killing over 3,500 in 1858. Norfolk, VA was only struck once in 1855. Since yellow fever never struck Norfolk during milder years, the population lacked immunity and approximately 10 percent of the city died in 1855. Charleston and Mobile show similar sporadic patterns. Likely due to the Union’s naval blockade, yellow fever did not visit any American port cities in large numbers during the Civil War.
Immigrants were particularly prone to yellow fever because they often came from European countries rarely visited by yellow fever. Native New Orleanians, however, typically caught yellow fever during a mild year as children and were then immune to the disease for the rest of their lives. For this reason, yellow fever earned the name the “stranger’s disease.”
Data from the full count of the 1880 census show that yellow fever fatality rates during an individual’s year of birth negatively affected adult occupational status, but only for individuals with foreign-born mothers. Those with US-born mothers were relatively unaffected by the disease. There are also effects for those who are exposed to yellow fever one or two years after their birth, but there are no effects, not even for those with immigrant mothers, when exposed to yellow fever three or four years after their births. These results suggest that early-life exposure to infectious disease, not just city-wide responses to disease, influence human capital development.
Martin Saavedra
