Airborne diseases: Tuberculosis in the Union Army
Home > Airborne diseases: Tuberculosis in the Union Army
by Javier Birchenall (University of California, Santa Barbara)
This is Part F of the Economic History Society’s blog series: ‘The Long View on Epidemics, Disease and Public Health: Research from Economic History’ The full article from this blog was published in ‘Explorations in Economic History’ and is available here

Tuberculosis (TB) is one of the oldest and deadliest diseases. Traces of TB in humans can be found as early as 9,000 years ago, and written accounts date back 3,300 years in India. Untreated, TB’s case-fatality rate is as high as 50 percent. It was a dreaded disease. TB is an airborne disease caused by the bacteria Mycobacterium tuberculosis. Tuberculosis spreads through the air when a person who has an active infection coughs, sneezes, speaks, or sings. Most cases remain latent and do not develop symptoms. Activation of tuberculosis is particularly influenced by undernutrition.
Tuberculosis played a prominent role in the secular mortality decline. Of the 27 years of life expectancy gained in England and Wales between 1871 and 1951, TB accounts for about 40 percent of the improvement, a 12-year gain. Modern medicine, the usual suspect used to explain this mortality decline, could not have been the culprit. As Thomas McKeown famously pointed out, TB mortality started its decline long before the tubercle bacillus was identified and long before an effective treatment was provided (Figure 1). McKeown viewed improvements in economic and social conditions, especially improved diets, as the principal factor arresting the combatting tuberculosis. A healthy diet, however, is not the only factor behind nutritional status. Infections, no matter how mild, reduce nutritional status and increase susceptibility to infection.
Figure 1. Mortality rate from TB.
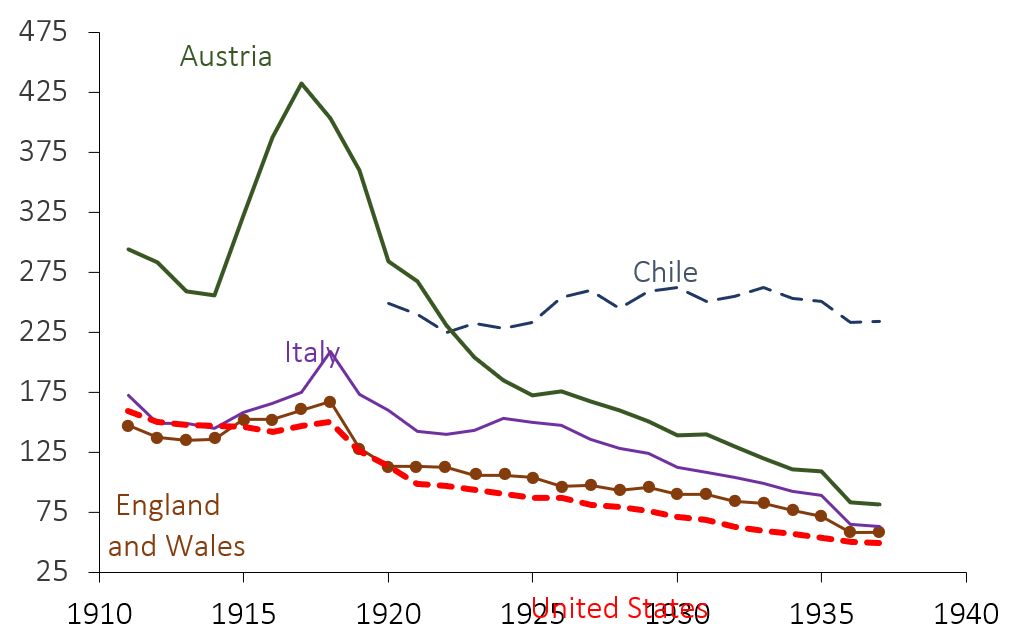
Source: as per original article
In “Airborne Diseases: Tuberculosis in the Union Army” I studied the determinants of diagnosis, discharge, and mortality from tuberculosis in the past. I examined the medical histories of 25,000 soldiers and veterans in the Union Army using data collected under the direction of Robert Fogel. The Civil War brought together soldiers from many socioeconomic conditions and ecological backgrounds into an environment which was ideal for the spread of this disease. The war also provided a unique setting to examine many of the factors which were likely responsible for the decline in TB mortality. Before enlistment, individuals had differential exposure to harmful dust and fumes. They also faced different disease environments and living conditions. By housing recruits in confined spaces, the war exposed soldiers to a host of waterborne and airborne infections. In the Civil War, disease was far more deadly than battle.
The Union Army data contains detailed medical records and measures of nutritional status. Height at enlistment measures net nutritional experiences at early ages. Weight, needed to measure current nutritional status using the Body Mass Index (BMI), is available for war veterans. My estimates use a hazard model and a variety of controls aligned with existing explanations proposed for the decline in TB prevalence and fatality rates. By how much would the diagnosis of TB have declined if the average Union Army soldier had the height of the current U.S. male population, and if all his relevant infections diagnosed prior to TB were eradicated? Figure 2 presents the contribution of the predictors of TB diagnosis in soldiers who did not engage in battle, and Figure 3 reports soldiers discharged because of TB. Nutritional experiences in early life provided a protective effect against TB. Between 25 and 50 per cent of the predictable decline in tuberculosis could be associated with the modern increase in height. Declines in the risk of waterborne and airborne diseases are as important as the predicted changes in height
Figure 2. Contribution of various factors to the decline in TB diagnosis
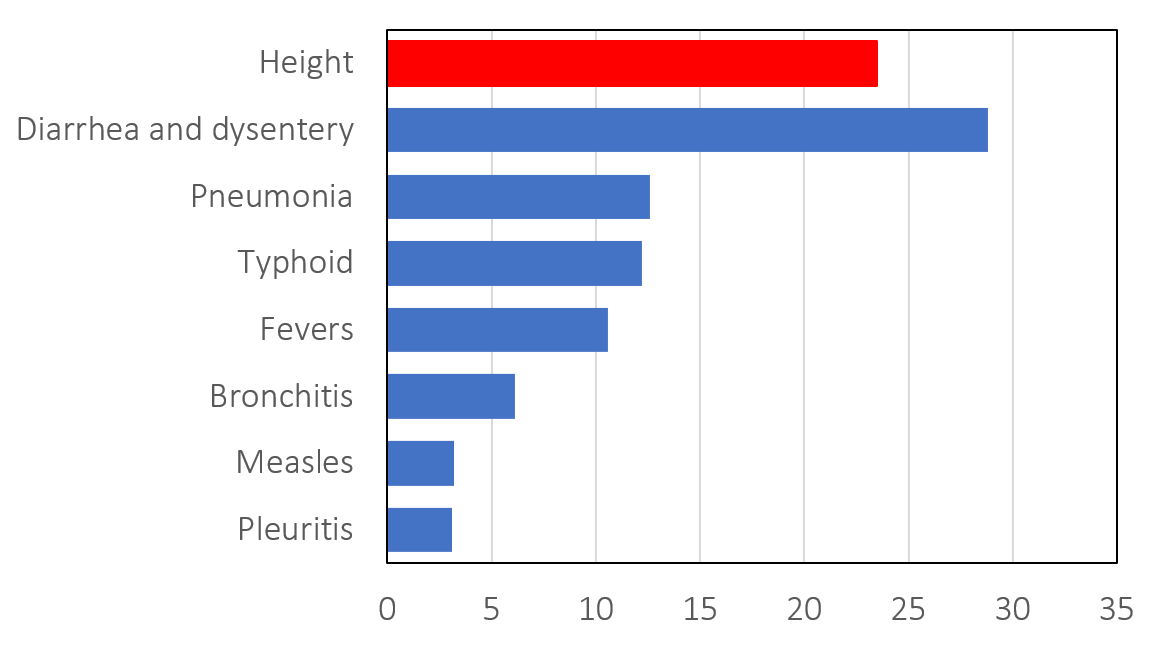
Figure 3. Contribution of various factors to the decline in discharges because of TB.

My analysis showed that a wartime diagnosis of TB increased the risk of tuberculosis mortality. Because of the chronic nature of the disease, infected soldiers likely developed a latent or persistent infection that remained active until resistance failed at old age. Nutritional status provided some protection against mortality. For veterans, height was not as robust as BMI. If a veteran’s BMI increased from its historical value of 23 to current levels of 27, his mortality risk from tuberculosis would have been reduced by 50 per cent. Overall, the contribution of changes in `pure’ diets and changes in infectious disease exposure, was probably equal.
What lessons can be drawn for the current covid-19 pandemic? Covid-19 is also an airborne disease. Airborne diseases (e.g., influenza, measles, smallpox, and tuberculosis) are difficult to control. In unfamiliar populations, they often break wreak havoc. But influenza, measles, smallpox, and tuberculosis are mostly killers from the past. The findings in my paper suggest that the conquest of tuberculosis happened through both individual and public health efforts. Improvements in diets and public health worked simultaneously and synergistically. There was no silver bullet to defeat the great white plague, tuberculosis. Diets are no longer as inadequate as in the past. Still, Covid-19 has exposed differential susceptibility to the disease. Success in combatting Covid-19 is likely to require simultaneous and synergistic private and public efforts.
